Investigating Accidents and Incidents:
Purpose:
Every year people are killed or injured at work. Over 40 million working days are lost annually through work-related accidents and illnesses. Recent figures show that an average of 250 employees and self-employed peopleare killed each year as a result of accidents in the workplace.1 A further 150 000 sustain major injuries or injuries that mean they are absent from work for more than three days. Over 2.3 million cases of ill health are caused or made worse by work.
 According to the Labour Force Survey, over 40 million working days are lost through work-related injuries and ill health, at a cost to business of £2.5 billion.
The same accidents happen again and again, causing suffering and distress to an ever-widening circle of workers and their families. The investigation and analysis of work-related accidents and incidents forms an essential part of managing health and safety. However, learning the lessons from what you uncover is at the heart of preventing accidents and incidents. Identify what is wrong and take positive steps to put it right. This guide will show you how.
Carrying out your own health and safety investigations will provide you with a deeper understanding of the risks associated with your work activities. Blaming individuals is ultimately fruitless and sustains the myth that accidents and cases of ill health are unavoidable when the opposite is true. Well thought-out risk control measures, combined with adequate supervision, monitoring and effective
According to the Labour Force Survey, over 40 million working days are lost through work-related injuries and ill health, at a cost to business of £2.5 billion.
The same accidents happen again and again, causing suffering and distress to an ever-widening circle of workers and their families. The investigation and analysis of work-related accidents and incidents forms an essential part of managing health and safety. However, learning the lessons from what you uncover is at the heart of preventing accidents and incidents. Identify what is wrong and take positive steps to put it right. This guide will show you how.
Carrying out your own health and safety investigations will provide you with a deeper understanding of the risks associated with your work activities. Blaming individuals is ultimately fruitless and sustains the myth that accidents and cases of ill health are unavoidable when the opposite is true. Well thought-out risk control measures, combined with adequate supervision, monitoring and effective
management (ie your risk management system) will ensure that your work activities are safe.
An effective investigation requires a methodical, structured approach to information gathering, collation and analysis. The findings of the investigation will form the basis of an action plan to prevent the accident or incident from happening again and for improving your overall management of risk.
Every year people are killed or injured at work. Over 40 million working days are lost annually through work-related accidents and illnesses. Recent figures show that an average of 250 employees and self-employed peopleare killed each year as a result of accidents in the workplace.1 A further 150 000 sustain major injuries or injuries that mean they are absent from work for more than three days. Over 2.3 million cases of ill health are caused or made worse by work.
According to the Labour Force Survey, over 40 million working days are lost through work-related injuries and ill health, at a cost to business of £2.5 billion.
The same accidents happen again and again, causing suffering and distress to an ever-widening circle of workers and their families. The investigation and analysis of work-related accidents and incidents forms an essential part of managing health and safety. However, learning the lessons from what you uncover is at the heart of preventing accidents and incidents. Identify what is wrong and take positive steps to put it right. This guide will show you how.
Carrying out your own health and safety investigations will provide you with a deeper understanding of the risks associated with your work activities. Blaming individuals is ultimately fruitless and sustains the myth that accidents and cases of ill health are unavoidable when the opposite is true. Well thought-out risk control measures, combined with adequate supervision, monitoring and effective
management (ie your risk management system) will ensure that your work activities are safe.
management (ie your risk management system) will ensure that your work activities are safe.
An effective investigation requires a methodical, structured approach to information gathering, collation and analysis. The findings of the investigation will form the basis of an action plan to prevent the accident or incident from happening again and for improving your overall management of risk.
language of investigation:

causes of adverse events:
Why investigate?


When should it start?
The urgency of an investigation will depend on the magnitude and immediacy of the risk involved (eg a major accident involving an everyday job will need to be investigated quickly).
In general, adverse events should be investigated and analysed as soon as possible. This is not simply good practice; it is common sense – memory is best and motivation greatest immediately after an adverse event. What does it involve?
An investigation will involve an analysis of all the information available, physical (the scene of the incident), verbal (the accounts of witnesses) and written (risk assessments, procedures, instructions, job guides etc), to identify what went wrong and determine what steps must be taken to prevent the adverse event from happening again.
It is important to be open, honest and objective throughout the investigation process. Pre-conceived ideas about the process, the equipment or the people involved in an adverse event may blind you to the real causes. Question everything. Be wary of blaming individuals.
What makes a good investigation?
To get rid of weeds you must dig up the root. If you only cut off the foliage, the weed will grow again.
What does it involve?
An investigation will involve an analysis of all the information available, physical (the scene of the incident), verbal (the accounts of witnesses) and written (risk assessments, procedures, instructions, job guides etc), to identify what went wrong and determine what steps must be taken to prevent the adverse event from happening again.
It is important to be open, honest and objective throughout the investigation process. Pre-conceived ideas about the process, the equipment or the people involved in an adverse event may blind you to the real causes. Question everything. Be wary of blaming individuals.
What makes a good investigation?
To get rid of weeds you must dig up the root. If you only cut off the foliage, the weed will grow again.
Similarly it is only by carrying out investigations which identify root causes that organisations can learn from their past failures and prevent future failures.
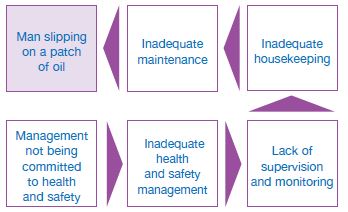
Simply dealing with the immediate causes of an adverse event may provide a shortterm fix. But, in time, the underlying/root causes that were not addressed will allow conditions to develop where further adverse events are likely, possibly with more serious consequences. It is essential that the immediate, underlying causes and root causes are all identified and remedied.
The objective is to establish not only how the adverse event happened, but more importantly, what allowed it to happen.
The root causes of adverse events are almost inevitably management, organisational or planning failures.
 Look carefully at your health and safety policy and how it is reflected in the workplace. Do staff understand the health and safety message in general and in particular those parts that relate to their work? Is something missing from the policy? Is it implemented, or is management failing to ensure that health and safety measures remain in place and are effective at all times? If not, your health and
Look carefully at your health and safety policy and how it is reflected in the workplace. Do staff understand the health and safety message in general and in particular those parts that relate to their work? Is something missing from the policy? Is it implemented, or is management failing to ensure that health and safety measures remain in place and are effective at all times? If not, your health and
safety policy needs to be changed.
The investigation should be thorough and structured to avoid bias and leaping to conclusions. Don’t assume you know the answer and start finding solutions before you complete the investigation. A good investigation involves a systematic and structured approach.
The urgency of an investigation will depend on the magnitude and immediacy of the risk involved (eg a major accident involving an everyday job will need to be investigated quickly).
In general, adverse events should be investigated and analysed as soon as possible. This is not simply good practice; it is common sense – memory is best and motivation greatest immediately after an adverse event.
What does it involve?
An investigation will involve an analysis of all the information available, physical (the scene of the incident), verbal (the accounts of witnesses) and written (risk assessments, procedures, instructions, job guides etc), to identify what went wrong and determine what steps must be taken to prevent the adverse event from happening again.
It is important to be open, honest and objective throughout the investigation process. Pre-conceived ideas about the process, the equipment or the people involved in an adverse event may blind you to the real causes. Question everything. Be wary of blaming individuals.
What makes a good investigation?
To get rid of weeds you must dig up the root. If you only cut off the foliage, the weed will grow again.
Similarly it is only by carrying out investigations which identify root causes that organisations can learn from their past failures and prevent future failures.
Similarly it is only by carrying out investigations which identify root causes that organisations can learn from their past failures and prevent future failures.
Simply dealing with the immediate causes of an adverse event may provide a shortterm fix. But, in time, the underlying/root causes that were not addressed will allow conditions to develop where further adverse events are likely, possibly with more serious consequences. It is essential that the immediate, underlying causes and root causes are all identified and remedied.
The objective is to establish not only how the adverse event happened, but more importantly, what allowed it to happen.
The root causes of adverse events are almost inevitably management, organisational or planning failures.
Look carefully at your health and safety policy and how it is reflected in the workplace. Do staff understand the health and safety message in general and in particular those parts that relate to their work? Is something missing from the policy? Is it implemented, or is management failing to ensure that health and safety measures remain in place and are effective at all times? If not, your health and
safety policy needs to be changed.
safety policy needs to be changed.
The investigation should be thorough and structured to avoid bias and leaping to conclusions. Don’t assume you know the answer and start finding solutions before you complete the investigation. A good investigation involves a systematic and structured approach.
Information gathering:

Analysis:
Risk control measures:
Action plan and implementation:
RIDDOR:
For those accidents and dangerous occurrences that are reportable under the provisions of RIDDOR (the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995), this information must be notified to the enforcing authority.
- keeping a copy of the form;
- recording the incident in the accident book;
- recording the incident electronically.
For those accidents and dangerous occurrences that are reportable under the provisions of RIDDOR (the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995), this information must be notified to the enforcing authority.
- keeping a copy of the form;
- recording the incident in the accident book;
- recording the incident electronically.
The investigation:



An analysis involves examining all the facts, determining what happened and why. All the detailed information gathered should be assembled and examined to identify what information is relevant and what information is missing. The information gathering and analysis are actually carried out side by side. As the analysis progresses, further lines of enquiry requiring additional information will develop.
To be thorough and free from bias, the analysis must be carried out in a systematic way, so all the possible causes and consequences of the adverse event are fully considered. A number of formal methods have been developed to aid this approach. One useful method for organising your information, identifying gaps and beginning the analysis is Events and Causal Factor Analysis (ECFA), which is beyond the scope of this guidance.
The analysis should be conducted with employee or trade union health and safety representatives and other experts or specialists, as appropriate. This team approach can often be highly productive in enabling all the relevant causal factors to emerge.
One useful method for organising your information, identifying gaps and beginning the analysis is Events and Causal Factor Analysis (ECFA), which is beyond the scope of this guidance.
The analysis should be conducted with employee or trade union health and safety representatives and other experts or specialists, as appropriate. This team approach can often be highly productive in enabling all the relevant causal factors to emerge.
An analysis involves examining all the facts, determining what happened and why. All the detailed information gathered should be assembled and examined to identify what information is relevant and what information is missing. The information gathering and analysis are actually carried out side by side. As the analysis progresses, further lines of enquiry requiring additional information will develop.
To be thorough and free from bias, the analysis must be carried out in a systematic way, so all the possible causes and consequences of the adverse event are fully considered. A number of formal methods have been developed to aid this approach.
One useful method for organising your information, identifying gaps and beginning the analysis is Events and Causal Factor Analysis (ECFA), which is beyond the scope of this guidance.
The analysis should be conducted with employee or trade union health and safety representatives and other experts or specialists, as appropriate. This team approach can often be highly productive in enabling all the relevant causal factors to emerge.




No comments:
Post a Comment